

Signs & Symptoms of MSMDS
WHAT ARE THE SIGNS & SYMPTOMS
OF MULTISYSTEMIC SMOOTH MUSCLE DYSFUNCTION SYNDROME?
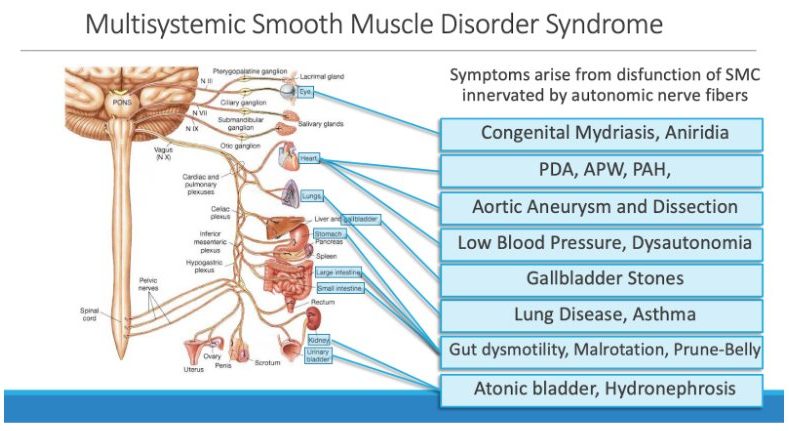
Figure 3. Organ Dysfunctions Reported on Patients with MSMDS
The three hallmark signs of MSMDS include
Patent Ductus Arteriosus (PDA) or Aortopulmonary (APW), Congenital Mydriasis, and White Matter Changes. When two of these three signs are present, genetic testing should be performed. In addition, pulmonary arterial hypertension (PAH), chronic lung disease, vascular disease and aortic dissection, white matter injury, stroke due to cerebrovascular disease, intestinal involvement, and atonic bladder are frequently present. Additional signs and symptoms may include other cardiac anomalies such as Aortic Coarctation, Atrial and/or Ventricular Septal Defect, stroke-like symptoms including confusion, speech problems and temporary loss of sensation or movement, frequently feeling hot or cold (due to inability to self-regulate body temperature), and inability to get “chills.”
Patent Ductus Arteriosus or Aortopulmonary Window 4,5
- A patent ductus arteriosus (PDA) is an unclosed hole in the Aorta. After birth, the ductus arteriosus typically closes within the first few days. In babies with MSMDS, this closure does not occur extra blood gets pumped from aorta into the pulmonary (lung) arteries via the PDA . In a large PDA, the extra blood being pumped into the lung arteries makes the heart and lungs work harder and can cause congestion in the lungs and low oxygen levels. A PDA that does not close on its own typically requires surgical intervention. Aortopulmonary (AP) window is a rare heart defect in which there is a hole connecting the the aorta and the pulmonary artery near the heart. As with large PDAs, blood from the aorta flows into the pulmonary artery, and as a result too much blood flows to the lungs. This causes low blood oxygen levels, high blood pressure in the lungs (pulmonary hypertension), and leads to congestive heart failure.
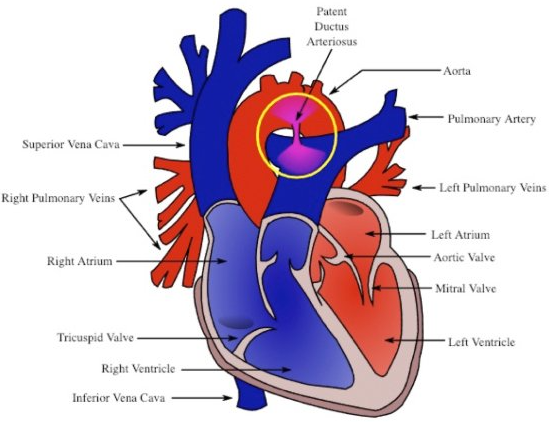
Figure 4. Heart Cross Section with Patent Ductus Arteriosus (PDA)
Congenital Mydriasis 6
- Congenital Mydriasis is the appearance of fixed and dilated pupils. In normal eyes, the pupils constrict and dilate to filter light. In the case of congenital mydriasis, the pupils are unable to constrict to block excess light. Congenital mydriasis in the presence of MSMDS may sometimes be mistaken for Aniridia or partial Aniridia. Specific to MSMDS, the smooth muscle function of the iris muscles is disrupted, creating a scalloped, wisping pupillary margin.

Figure 5. Iris Hypoplasia Resulting in Scalloped Pupillary Margin
Pulmonary Arterial Hypertension (PAH) 7
- Pulmonary Hypertension refers to abnormally high blood pressure in the blood vessels between the lungs and heart. When the pressure becomes too high, the arteries in the lungs narrow, reducing blood flow through the lungs and causing low levels of oxygen in the blood. The exact mechanism of disease in MSMDS is not well understood, however is suspected to be caused by vascular anomalies and some degree of interstitial lung disease. Left untreated, PAH can lead to irreversible heart damage and/or heart failure.
Aortic Aneurysms and Vascular Disease
- The lining of arteries and vessels in the human body contains smooth muscle that regulates dilation and constriction for multiple processes in the body. In MSMDS, these arteries and vessels are unable to widen and narrow to control body temperature and blood flow. Over time, the lack of regulation can lead to weakening in the arterial and vessel linings (aneurysms) and profound vascular disease including blocking of small vessels and rupture of large vessels and arteries. Also highly prevalent in this population are blood clots due to poor regulation of blood flow throughout the body and excess production of impaired smooth muscle cells. Patients must be monitored regularly throughout their lifetime to prevent Aortic Rupture (dissection) and assess for aneurysms throughout the body.
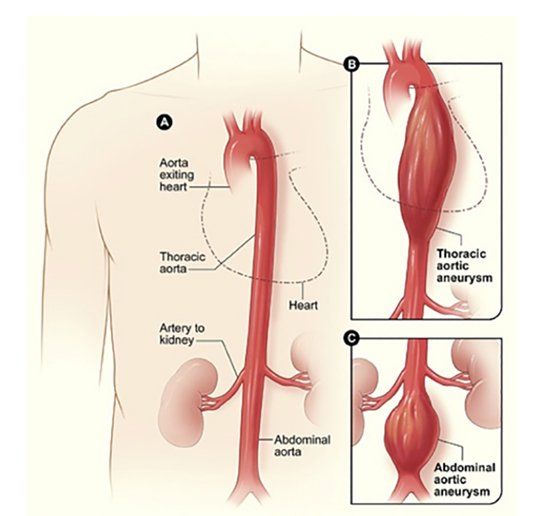
Figure 6. (A) Normal Aorta (B) Thoracic Aortic Aneurysm (C) Abdominal Aortic Aneurysm
Cerebrovascular Disease, White Matter Injury and Stroke 8
- Cerebrovascular disease refers to disease of the vasculature (arteries and veins) of the brain in which the blood vessels are impacted by a pathological process or disease. Brain changes are seen as early as birth in MSMDS in the form of white matter injury often diagnosed after an MRI of the brain is performed. As the disease progresses, smaller arteries/vessels begin to become increasingly more narrow due to excess production of impaired smooth muscle cells and connective tissue released around them. These narrowed vessels are at higher risk of clot occlusion due to their abnormal blood flow. The narrowed small vessels of the brain are also in charge of distributing the blood flow and making sure the brain ALWAYS gets blood to where it needs (i.e. to the speech area when talking). This function of the brain vessels is called autoregulation and is accomplished by smooth muscle contraction and relaxation in the vessel wall. In MSMDS, this autoregulation is impaired and can lead to brain tissue injury (stroke, white matter disease) or Transient Ischemic Attacks (TIAs) when the blood pressure is too low (i.e during severe dehydration and anesthesia). As the larger arteries (elastic arteries) widen throughout the body, decreased blood flow creates increased risk of blood clots, which can then travel to the brain. This causes TIAs if the flow is restored or strokes (brain tissue damage) when the decreased flow is not normalized in time.
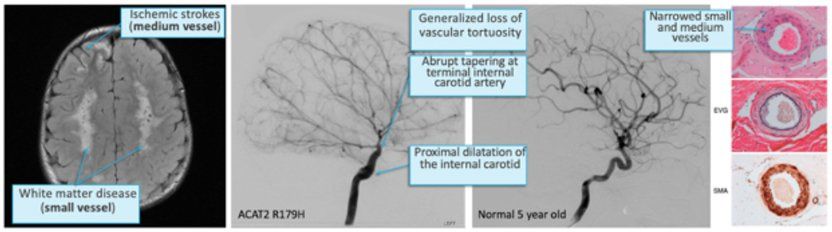
Figure 7. MRI of the brain (left) with white matter injury and small ischemic infarct. Catheter angiogram (middle) comparing ACTA2 R179H straight and narrowed vessels with an age matched non-affected child. Far right panel shows histological abnormalities seen in medium size vessels and was adapted from Georgescu et al, 2015.19
Intestinal Hypoperistalsis (Gut Dysmotility) and Malrotation 9
- Intestinal rotation occurs while a fetus is forming in the uterus. Malrotation occurs when the intestine does not make the turns as it should. A volvulus can also occur after birth, where the intestine becomes twisted. Intestinal malrotations and volvuli can cause life-threatening bowel obstructions. Frequently in MSMDS, malrotations and/or volvuli are present in the intestines and stomach. Gut dysmotility is also prevalent in those with MSMDS due to dysfunction of the smooth muscle apparatus that propels food forward through the digestive tract. Intestinal malrotation, volvuli, and gut dysmotility problems range from poor nutrition to life-threatening disease that may require surgical correction. Those affected should be monitored closely if any signs/symptoms of intestinal blockage occur such as vomiting, abdominal pain, or diarrhea/constipation.
Atonic/Hypotonic Bladder
- Those affected by MSMDS have impaired ability to completely expel urine from the bladder due to the lack of functional smooth muscle in the bladder lining. The inability to empty the bladder leads to bladder distention and frequent urinary tract infections (UTIs) that must be managed medically to prevent systemic infection.
Causes
- MSMDS is considered to be an autosomal dominant disease. In humans, every gene in our body has two copies that we inherit from each of our biological parents. In autosomal dominant diseases, although both gene copies are present, only one is expressed. ACTA2 mutations are considered autosomal dominant given that a mutation in only one of the two copies is sufficient to cause disease. In MSMDS, the intact copy of the gene is overridden by the mutated copy of the gene and is therefore not expressed.
Figure 8
*Not all patients experience the same presentation and challenges. Listed above are those that have been described to date for informational purposes only.
